Overview
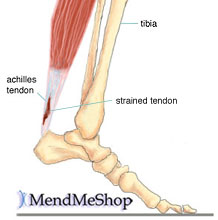 An Achilles tendon rupture is also known as a rupture of the gastrocnemius tendon, or the common calcanean tendon. The tendon is actually composed of 5 different tendons, the two most important being the superficial digital flexor and gastrocnemius tendons. The gastrocnemius tendon is the largest of these, and is the most powerful extensor of the hock (ankle) joint. Both the superficial digital flexor and gastrocnemius tendons attach to the heel bone, called the calcaneus bone. A rupture of the Achilles tendon may be a partial tear, which means just the gastrocnemius is torn, or a complete tear, in which all five tendons have been torn. (show diagrams, normal anatomy vs partial vs complete tears).
An Achilles tendon rupture is also known as a rupture of the gastrocnemius tendon, or the common calcanean tendon. The tendon is actually composed of 5 different tendons, the two most important being the superficial digital flexor and gastrocnemius tendons. The gastrocnemius tendon is the largest of these, and is the most powerful extensor of the hock (ankle) joint. Both the superficial digital flexor and gastrocnemius tendons attach to the heel bone, called the calcaneus bone. A rupture of the Achilles tendon may be a partial tear, which means just the gastrocnemius is torn, or a complete tear, in which all five tendons have been torn. (show diagrams, normal anatomy vs partial vs complete tears).
Causes
Ruptured Achilles tendons may result from falling from a height or down a hole. Increasing training intensity abruptly, boosting distance, frequency or duration by more than 10% a week. Failing to stretch before and after exercise. Repetitive training, especially uphill running. Deyhydration, which causes cramping and tightness in the calves. Taking antibiotics. Improper footwear. Explosive movements in competitive sports like basketball, soccer or track & field.
Symptoms
Patients with an Achilles tendon rupture will often complain of a sudden snap in the back of the leg. The pain is often intense. With a complete rupture, the individual will only be ambulate with a limp. Most people will not be able to climb stairs, run, or stand on their toes. Swelling around the calf may occur. Patients may often have had a sudden increase in exercise or intensity of activity. Some patients may have had recent corticosteroid injections or use of fluoroquinolone antibiotics. Some athletes may have had a prior injury to the tendon.
Diagnosis
Diagnosis is made by clinical history; typically people say it feels like being kicked or shot behind the ankle. Upon examination a gap may be felt just above the heel unless swelling has filled the gap and the Simmonds' test (aka Thompson test) will be positive; squeezing the calf muscles of the affected side while the patient lies prone, face down, with his feet hanging loose results in no movement (no passive plantarflexion) of the foot, while movement is expected with an intact Achilles tendon and should be observable upon manipulation of the uninvolved calf. Walking will usually be severely impaired, as the patient will be unable to step off the ground using the injured leg. The patient will also be unable to stand up on the toes of that leg, and pointing the foot downward (plantarflexion) will be impaired. Pain may be severe, and swelling is common. Sometimes an ultrasound scan may be required to clarify or confirm the diagnosis. MRI can also be used to confirm the diagnosis.
Non Surgical Treatment
Nonsurgical method is generally undertaken in individuals who are old, inactive, and at high-risk for surgery. Other individuals who should not undergo surgery are those who have a wound infection/ulcer around the heel area. A large group of patients who may not be candidates for surgery include those with diabetes, those with poor blood supply to the foot, patients with nerve problems in the foot, and those who may not comply with rehabilitation. Nonsurgical management involves application of a short leg cast to the affected leg, with the ankle in a slightly flexed position. Maintaining the ankle in this position helps appose the tendons and improves healing. The leg is placed in a cast for six to 10 weeks and no movement of the ankle is allowed. Walking is allowed on the cast after a period of four to six weeks. When the cast is removed, a small heel lift is inserted in the shoe to permit better support for the ankle for an additional two to four weeks. Following this, physical therapy is recommended. The advantages of a nonsurgical approach are no risk of a wound infection or breakdown of skin and no risk of nerve injury. The disadvantages of the nonsurgical approach includes a slightly higher risk of Achilles tendon rupture and the surgery is much more complex if indeed a repair is necessary in future. In addition, the recuperative period after the nonsurgical approach is more prolonged.
Surgical Treatment
A completely ruptured Achilles tendon requires surgery and up to 12 weeks in a cast. Partial tears are sometimes are treated with surgery following by a cast. Because the tendon shortens as it heals, a heel lift is used for 6 months or more after the cast comes off. Physical therapy to regain flexibility and then strength are begun as soon as the cast is off.
An Achilles tendon rupture is also known as a rupture of the gastrocnemius tendon, or the common calcanean tendon. The tendon is actually composed of 5 different tendons, the two most important being the superficial digital flexor and gastrocnemius tendons. The gastrocnemius tendon is the largest of these, and is the most powerful extensor of the hock (ankle) joint. Both the superficial digital flexor and gastrocnemius tendons attach to the heel bone, called the calcaneus bone. A rupture of the Achilles tendon may be a partial tear, which means just the gastrocnemius is torn, or a complete tear, in which all five tendons have been torn. (show diagrams, normal anatomy vs partial vs complete tears).Causes
Ruptured Achilles tendons may result from falling from a height or down a hole. Increasing training intensity abruptly, boosting distance, frequency or duration by more than 10% a week. Failing to stretch before and after exercise. Repetitive training, especially uphill running. Deyhydration, which causes cramping and tightness in the calves. Taking antibiotics. Improper footwear. Explosive movements in competitive sports like basketball, soccer or track & field.
Symptoms
Patients with an Achilles tendon rupture will often complain of a sudden snap in the back of the leg. The pain is often intense. With a complete rupture, the individual will only be ambulate with a limp. Most people will not be able to climb stairs, run, or stand on their toes. Swelling around the calf may occur. Patients may often have had a sudden increase in exercise or intensity of activity. Some patients may have had recent corticosteroid injections or use of fluoroquinolone antibiotics. Some athletes may have had a prior injury to the tendon.
Diagnosis
Diagnosis is made by clinical history; typically people say it feels like being kicked or shot behind the ankle. Upon examination a gap may be felt just above the heel unless swelling has filled the gap and the Simmonds' test (aka Thompson test) will be positive; squeezing the calf muscles of the affected side while the patient lies prone, face down, with his feet hanging loose results in no movement (no passive plantarflexion) of the foot, while movement is expected with an intact Achilles tendon and should be observable upon manipulation of the uninvolved calf. Walking will usually be severely impaired, as the patient will be unable to step off the ground using the injured leg. The patient will also be unable to stand up on the toes of that leg, and pointing the foot downward (plantarflexion) will be impaired. Pain may be severe, and swelling is common. Sometimes an ultrasound scan may be required to clarify or confirm the diagnosis. MRI can also be used to confirm the diagnosis.
Non Surgical Treatment
Nonsurgical method is generally undertaken in individuals who are old, inactive, and at high-risk for surgery. Other individuals who should not undergo surgery are those who have a wound infection/ulcer around the heel area. A large group of patients who may not be candidates for surgery include those with diabetes, those with poor blood supply to the foot, patients with nerve problems in the foot, and those who may not comply with rehabilitation. Nonsurgical management involves application of a short leg cast to the affected leg, with the ankle in a slightly flexed position. Maintaining the ankle in this position helps appose the tendons and improves healing. The leg is placed in a cast for six to 10 weeks and no movement of the ankle is allowed. Walking is allowed on the cast after a period of four to six weeks. When the cast is removed, a small heel lift is inserted in the shoe to permit better support for the ankle for an additional two to four weeks. Following this, physical therapy is recommended. The advantages of a nonsurgical approach are no risk of a wound infection or breakdown of skin and no risk of nerve injury. The disadvantages of the nonsurgical approach includes a slightly higher risk of Achilles tendon rupture and the surgery is much more complex if indeed a repair is necessary in future. In addition, the recuperative period after the nonsurgical approach is more prolonged.
Surgical Treatment
A completely ruptured Achilles tendon requires surgery and up to 12 weeks in a cast. Partial tears are sometimes are treated with surgery following by a cast. Because the tendon shortens as it heals, a heel lift is used for 6 months or more after the cast comes off. Physical therapy to regain flexibility and then strength are begun as soon as the cast is off.
